
by Georgia Katsa, Georgia Koufioti, Eleni Koutzoukou, Athanasios Kounios
The Greek word “cannabis” was incorporated as such into Latin (cannabis) and with various modifications in French (canvre), Spanish (canamo), Portuguese (canhamo), Italian (canapa), Albanian (canep), Russian (konopli), Polish (konopi and penek), Syrian (kanabira), Arabic (Kannabb). Its entrance into the old (1000 AD) and modern English (as hanf and hemp, respectively), Belgian (kemp), German (hanf), Dutch (hennup), Swedish (hamp), Danish (hampa) etc. As a result it was established as a Hemp throughout the western world.
Botanical Classification
Clade: Rosids
Order: Rosales
Family: Cannabaceae
Genus: Cannabis
It is a reality that tolerance for pain ranges in different groups of people on the basis of physiology, psychology or even daily activity and education. From antiquity, pain was connected with conventional life from birth to death, natural or violent. People have historically had empirical ways to prevent pain through herbs or other methods. Pain, of course, can be regarded therapeutic and beneficial when it prevents inflammation or damage. There are a variety of therapeutic approaches to pain
These include passive and active treatment, medicine, behavioral therapy, psychological and a range of invasive procedures, such as surgery and other interventions. As pain symptoms vary from person to person, treatment management strategies should also be personalized. Medication alone is often not enough to handle pain, and sometimes overdose or excessive ingestion of drugs can often cause other problems.
In medieval times, pain relief was mainly based on a wide variety of herbs commonly available. The Middle Ages were renowned for the extensive use of pharmaceutical products. Quite important was the use of herbs containing opiate compounds where the patient could, in addition to relieve pain, also fall into a state of hypnosis.
It is known that man, in antiquity, sought medicines in nature. In the 1980s the endogenous opioid was first discovered and then the endogenous cannabinoid pain control system. Opium is a milky juice produced from the immature poppy fruit of the species Papaver Somniferum. The name opium comes from the ancient Greek word «οπός» (juice). From opium all exogenous (natural and synthetic) opiates come from. The first mention of his attributes was made by Theophrastus (300 BC), who called him Meconius. There is historical evidence that ancient Greeks and Romans knew many of the properties of opium and used it, among others, as an analgesic and anti-dysentery (anti-diarrhea). Paracelsus first introduced the tincture of opium (labdanum) for almost all types of medical problems, and later pharmacopoeia isolated morphine from opium. Around 1900, heroin was discovered and then many other synthetic opiates such as meperidine and methadone.
The center of pain lies in the brain and is triggered by the irritation of free nerve endings called alveolar receptors. Alveolar receptors are mainly found in the skin and mucous membranes and react to thermal, chemical or mechanical stimuli. The impulses are transmitted to the spinal cord by three types of fibers, Aβ, Aδ and C. Because Aβ and Aδ are covered by myelin, they transmit the painful stimulus more rapidly than C due to the fact that they are not covered by myelin transmits of pain. The stimuli from the Aδ / Aβ fibers produce pain that could be described as acute or diaphyseal, and the C, which occurs more slowly, produce pain that could be described as caustic or blunt and more diffuse.
The most common method of pain control is the use of analgesics and other medicines. Drug treatment may be beneficial in some patients with chronic pain, but is not universally effective. It is crucial that each person is able to respond differently to a drug substance. In addition, in certain people, the use of painkillers can exacerbate their symptoms over time or cause additional or dangerous side effects.
There are four major groups of medications used to treat pain and, in particular, chronic pain. Opioids are substances of plant or synthetic origin that bind to opioid receptors and exhibit partial agonistic action, such as morphine, codeine, methadone, butorphanol. The Greek pharmaceutical system is subject to specific legal classifications in accordance with Law 3459/2006.
- Non-opioids: aspirin, non-steroidal anti-inflammatory and acetaminophen
- Opioids: include but are not limited to morphine, codeine, hydrocodone, oxycodone and methadone. (Tramadol and tapentadol are not considered opioids, but they work primarily on the same receptors as opioids.)
- Ancillary analgesics: medicines that were originally used to treat pain disorders but are now also used to relieve pain in specific categories such as certain antidepressants and antipsychotics.
- Others: medicines without immediate pain relief properties that can be prescribed as part of this pain management plan. These include medications to treat insomnia, anxiety, depression and muscle spasms.
In cases of withdrawal of opioid withdrawal, various symptoms can occur such as: insomnia, anxiety, sweating, stomach cramps, nausea, vomiting, diarrhea, flu-like symptoms, muscle cramps. Prescription drugs that can help reduce the symptoms of opioid withdrawal include: clonidine (the patient should be monitored for blood pressure), muscle relaxants (methocarbamol, lioresal), dicyclomine, antidepressant, tranquilizers.
Non-steroidal anti-inflammatory drugs (NSAIDs) are widely used to treat pain and to manage edema and tissue damage that can result from inflammatory disease such as arthritis. A significant number of these drugs have antipyretic activity in addition to analgesic and anti-inflammatory effects and express their therapeutic effect by suppressing the biosynthesis of prostaglandins. Some of the primary indications for NSAID therapy include rheumatoid arthritis, osteoarthritis, dysmenorrhea. Their main mechanism of action is the inhibition of prostaglandin synthesis, but some also inhibit cyclooxygenases, enzymes that catalyze the synthesis of cyclic endoperoxides to form prostaglandins. They are usually less expensive than other formulations.
Drug administration can be carried out in a variety of ways such as per os (orally), by simply injecting the drug, transmucosal, by catheter placement, with a range of 2-6 blockades, with local anesthetics, with various blocking techniques for example arm or lumbar mesh or by cross-channel access. The cannabis genus is usually classified into three distinct types of plants: Cannabis sativa, Cannabis indica and Cannabis ruderalis. These historically correspond to the cultivated, the Indian and the native (Asian) variety of the plant respectively. In Greece it exists as a native and cultivated plant and has been known since antiquity. It is considered a fiber plant since it, in particular Sativa, receives fibers used for weaving and making cords, canvas and other materials. Its cultivation in Greece for the production of such species was a flourishing agricultural industry but was banned by Law 2107 of 11-3-1920. It is widely used all over the world as a drug and is permitted for use in medical problems in 8 countries. The natural cannabinoids come from the Cannabis sativa plant. The most important cannabinoids with studied biological effects are tetrahydro-cannabinol, cannabidol, cannabidiol, and cannabigerol. Many of the pharmacological effects of exogenous cannabinoids have been empirically known for centuries, with the first written mention being in the books of a Chinese emperor in 1400 BC. Endogenous cannabinoids are products of the cell membrane phospholipids, where phospholipase D results in the amantamide sequence and phospholipase C / A1 activates the glycerol 2-arachidonyl series. These endogenous cannabinoids in the peripheral blood and extracellular space circulate associated with an unknown, possibly protein carrier, and are transported to the cannabinoid receptors (CBR) to exert their action. An amount of it enters the cells where by the action of the enzymes the fatty acid amide hydrolase-A (A-AMH) for amantamide and the AMH for 2-AG are cleaved into arachidonate, ethanolamine and glycerol. Experiments and clinical studies have summarized that: cannabinoids have potent analgesic effects in models of tonic pain, hyperalgesic, with an inflammatory response in addition to thermal or diastolic stimulation. From such experiments it was found e.g. the better analgesic effect of some cannabinoids (Δ9-THC) in abdominal distal pain (intestinal pain) compared to non-tonic acute pain.
The therapeutic utility of cannabis and its producers is proven and accepted for the following wide range of pathological conditions:
1. Glaucoma (intraocular hypertension)
2. Side effects of chemotherapy (nausea and vomiting)
3. Asthma
4. Epilepsy and convulsions
5. Depression, anxiety, anorexia
6. Pain of various reasons
7. Malignant neoplasms
8. Dependence on opiates and alcohol.
Cannabis also has four major benefits that make it unique from a therapeutic point of view:
1. It is the most toxic of the available medicines.
2. It has a wide range of therapeutic applications.
3. Act through mechanisms that are different from those of other drugs.
4. It can be effectively and safely combined with any medicine (Picton, 2003)
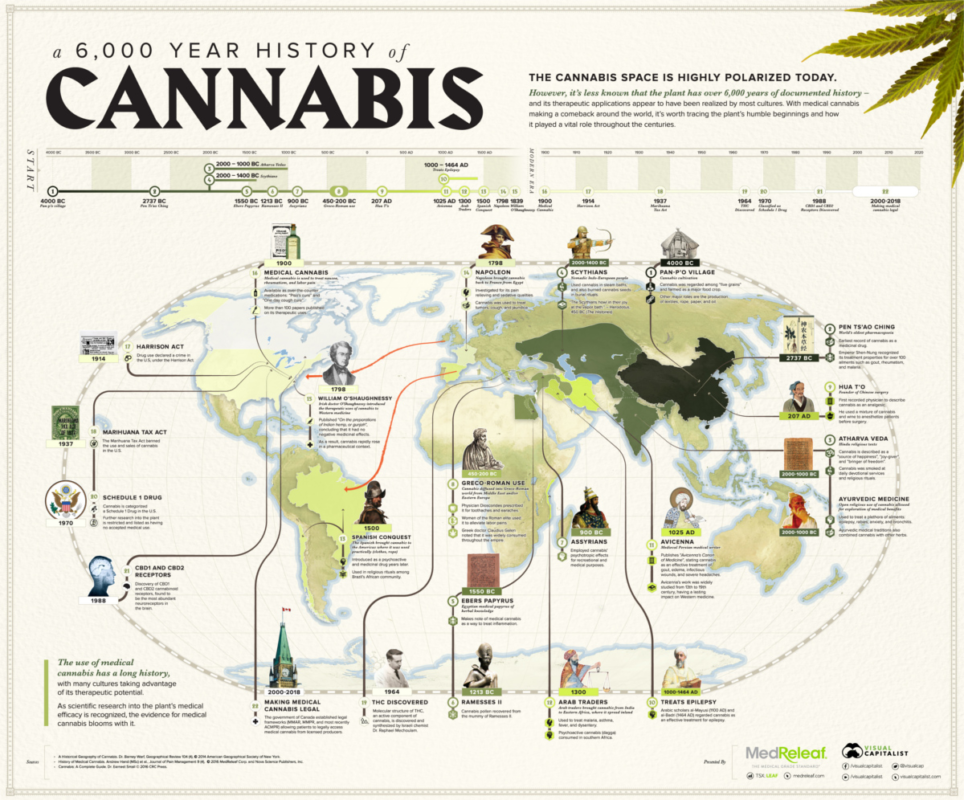
Many countries around the world as shown in the map below have stringent cannabis laws in contrary to others were not only cannabis is legal for medical use but also for all purposes of consumption.

In Greek reality, Section 1 of the Law 4523/2018 on the production of Cannabis Pharmaceutical products introduces an exception to paragraph 2 of Article 2 of Law 4139/2013 “on addictive substances and other provisions”, which relates to the substances in Schedule B of paragraph 2 of Article 1 of Law 4139/2013. Regulation (EC) No 3459/2006 as regards cannabis varieties of Cannabis Sativa L with a tetrahydrocannabinol (THC) content exceeding 0,2%. As specified in the Explanatory Memorandum, this exemption provides strict criteria to natural and legal persons for the production of Cannabis Sativa L with a tetrahydrocannabinol (THC) content of more than 0,2 per cent solely for the production of finished pharmaceutical products of cannabis for the supply of those to the state monopoly and for the supply or export to patients for medical purposes.

Moreover, this legal framework may arise a lot of benefits and may include the possibility of access of the patients to the final products of cannabis, given the therapeutic properties of cannabis in specific cases, generate new employment opportunities that will contribute to the development of the state of the art economy, taking advantage of the country’s competitive and efficient advantages and finally to create Economic benefits for the state from the export of cannabis finished products and the taxation of the economic activities of the industry, provided that the global market for the production and processing of medical cannabis is at an early stage of development.

Acknowledgements
We are grateful to the authors for kindly providing the original article.
 (No Ratings Yet)
(No Ratings Yet)